Aktuellt

Utbildning om Astma & KOL – När är det dags att göra mer?
Terapiinriktad utbildning med produktinformation i samband med ASTA-dagarna 2026.
Läs mer
Vill du veta det senaste inom luftvägar?
Vi sammanfattar höjdpunkterna från kongresser åt dig! Inom Chiesis nordiska medicinska team har vi flera personer med fokus på astma-KOL. Vi håller oss uppdaterade och delar gärna höjdpunkterna från kongresser
Läs mer
Sammanfattning av lungan genom livet – en nationell utbildningsdag
Vilka faktorer från födelse, eller kanske ännu tidigare, till vuxen ålder spelar roll för de tillstånd och sjukdomar som senare kan leda till KOL?
Läs mer
Inhalationsteknik är en färskvara
En studie med svenska KOL-patienter från 2021 visade att totalt 66 procent av patienterna i studien inte tog sin inhalation på rätt sätt och att ju fler inhalatorer patienterna hade,
Läs mer
Patientfall med kangrelor
Här kan du ta del av tre intressanta patientfall med kangrelor, framtagna i samarbete med överläkaren och interventionskardiologen Per Grimfjärd, MD, PhD vid Region Västmanland (engelskt tal). Gå till Kardiologi
Läs merWebinarer

Exacerbationer
Webbinarium KOL – exacerbationer Varför är det viktigt att undvika exacerbationer? Vilka verktyg kan man använda sig av för att bedöma grad av exacerbation? Är dyspné en prediktor för kommande
OBS utbildningsserie
Se mer
Fysisk aktivitet vid KOL – vikten av träning i teori och praktik
Denna utbildning syftar till att dels förklara vad som händer i kroppen och varför fysisk aktivitet ger så positiva effekter hos personer med KOL.
Läs mer
KOL-exacerbationer -mer akut än man kan tro
En KOL-exacerbation är inte bara en försämringsepisod av KOL, utan även potentiellt farligt tillstånd i behov av akut omhändertagande. I den här utbildningen får ni lära er mer om diagnostik, behandling och eventuella konsekvenser av exacerbationer och hur dessa bäst kan förebyggas.
Läs mer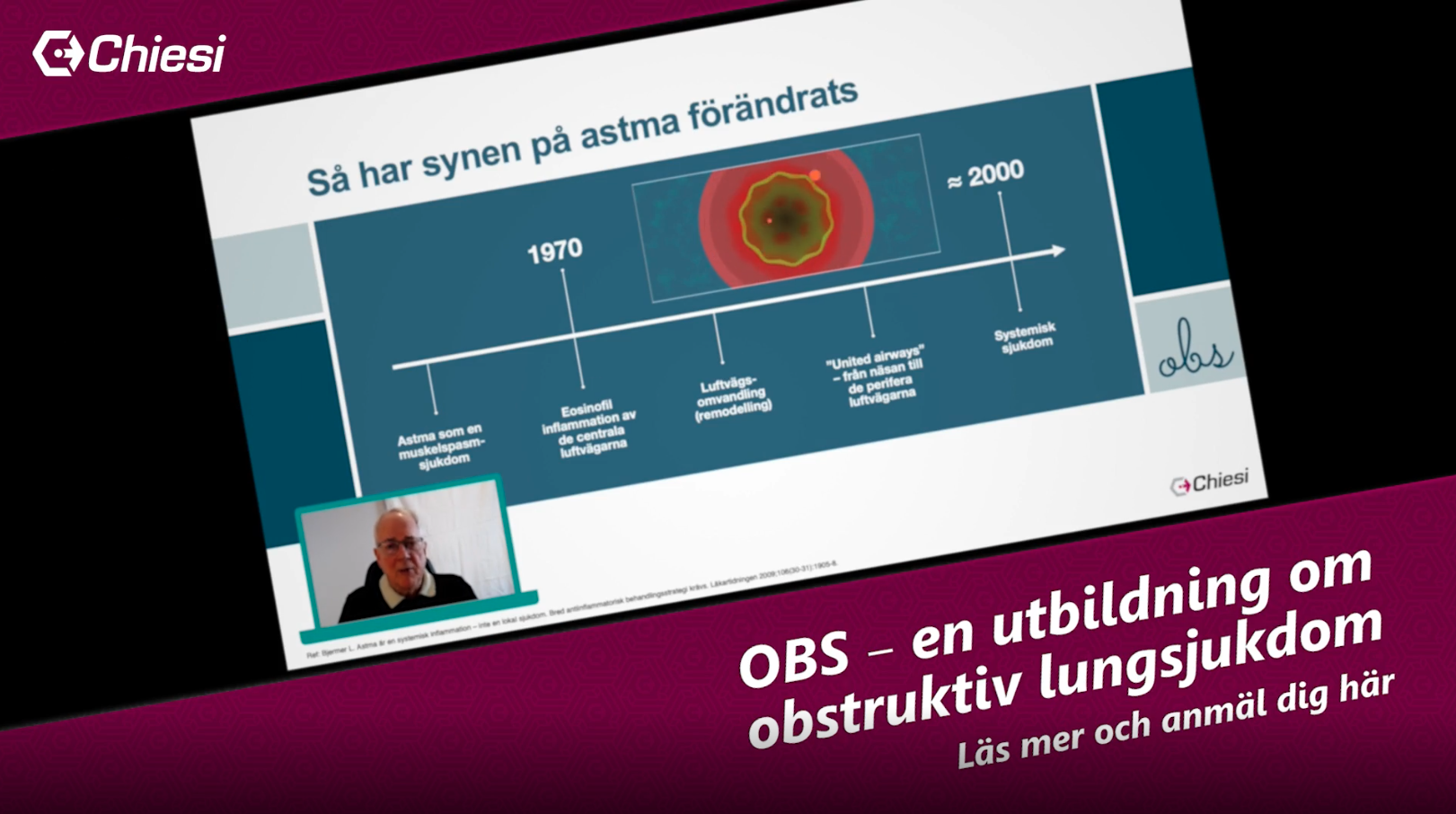
Astma och perifera luftvägar
Vilken inverkan har de små luftvägarna vid astma och hur bör behandlingen se ut?
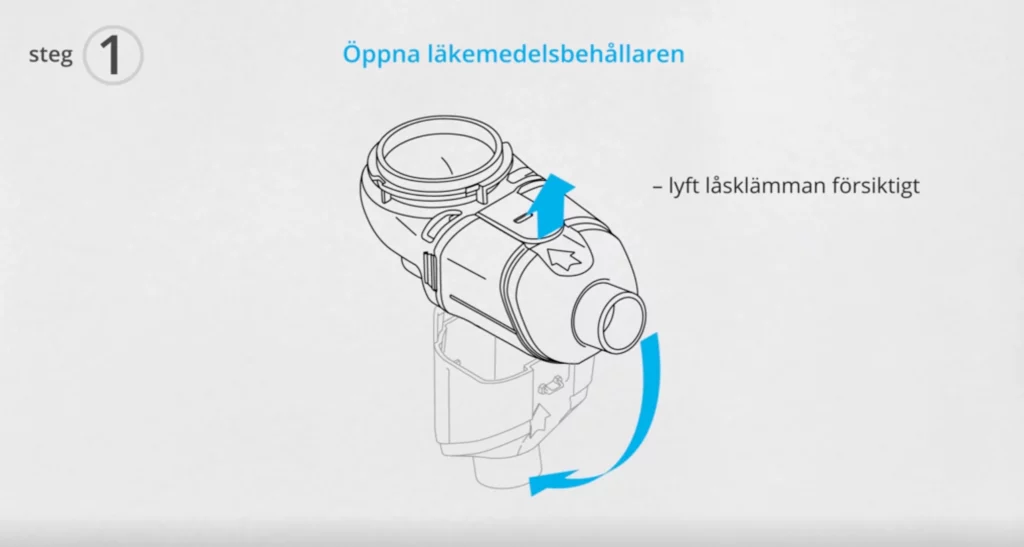
Läs merInstruktionsfilmer
Se alla Instruktionsfilmer